PPD is one of the most common medical conditions associated
with pregnancy,1 yet it is underdiagnosed and undertreated1-3

About 1 in 8 women report experiencing symptoms of
postpartum depression after giving birth4

Risk factors
Women often have numerous and overlapping factors that may compound risk for PPD1,5
Biological1,6-8*
- Personal and family history of depression
- Sleep disturbances
- Hormonal changes
- Genetics
Environmental1,9,10*
- Stressful life events
- Childcare stress
- Partner violence
Obstetric5,11,12*
- Obstetric complications
- Traumatic birth experience
- Difficulty breastfeeding
Psychosocial1,5*
- Lack of social support
- Race (as a social construct)
- Employment status
- Socioeconomic status
- Pregnancy intendedness
*Not an all-inclusive list of risk factors associated with PPD.
Any woman can be at risk for PPD13
Symptoms
PPD symptom onset can occur during or after pregnancy1,14
While PPD symptoms may look like the baby blues, there are key differences5
Baby blues symptoms peak around 5 days postpartum and resolve within 2 weeks5,13
PPD symptoms are present for at least 2 weeks and cause significant distress or functional impairment1,14
Patients with a PPD diagnosis may be struggling with persistent symptoms that can be debilitating1,13,14
Mood5,13,14
- Persistent sad or “empty” mood
- Loss of interest or pleasure in daily activities
- Irritability or frustration
- Feelings of worthlessness or guilt
- Hopelessness or pessimism
- Anxiety or obsessive thinking
- Feeling overwhelmed
- Uncontrollable anger
- Thoughts of death, suicide attempts, or self-harm
Cognitive13,14
- Impaired ability to think or concentrate
- Difficulty making decisions
- Memory problems
Somatic/psychomotor13,14
- Difficulty sleeping, waking early, or oversleeping
- Restlessness or having trouble sitting still
- Abnormal changes in weight or appetite
- Fatigue or abnormal decrease in energy
Infant-related13
- Trouble bonding or forming an attachment with the baby
- Persistent doubts about ability to care for the baby
- Thoughts of infant-related harm
Provide your patients with this guide to help them talk about depressive symptoms they may be experiencing

Screening
Screening early and often may support timely intervention1
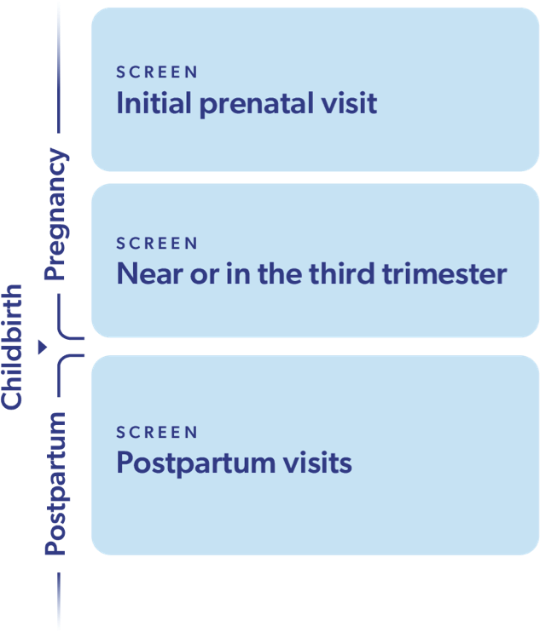
ACOG recommends screening for depressive symptoms at multiple timepoints1
Patients should be screened for depressive symptoms at multiple timepoints during pregnancy and after delivery
using standardized and validated instruments like the EPDS or PHQ-91


About 50%
of women with a PPD diagnosis began experiencing depressive symptoms during pregnancy14
ACOG, American College of Obstetricians and Gynecologists; EPDS, Edinburgh Postnatal Depression Scale; PHQ-9, Patient Health Questionnaire-9.
ACOG recommends screening for bipolar disorder before initiating pharmacotherapy for depression, if not previously done.1
ACOG recommends consideration of zuranolone for treatment of postpartum depression15
ACOG recommends consideration of zuranolone in the postpartum period (ie, within 12 months postpartum) for depression that has onset in the third trimester or within 4 weeks postpartum. The decision to use zuranolone should balance the benefits with the risks and challenges.15
Explore ZURZUVAE efficacy outcomes from a 6-week clinical study
Learn about the 3 steps needed to start your patients with PPD on ZURZUVAE